
Artwork by Greg A. Dunn
After what you could call a professionally-induced hiatus, I am glad to share some fresh thoughts regarding the healthcare space. This continues to be an extraordinarily vibrant time for BioPharma, and I hope to post more frequently over the coming months.
The following is an extensive write-up, so I’ve prefaced it with an index below.
The post is also peppered with references to scientific literature, which are appended via footnotes.
- Why I care
- The challenge of treatment-refractory status epilepticus
- New findings around the efficacy of second-line therapy
- Incidence of SE and RSE
- A succinct discussion of available 2nd and 3rd line AEDs and their limitations
- Rapid seizure cessation, durable efficacy and lack of systemic toxicity: a paradigm shift is at hand
- Ganaxolone’s MOA, PK/PD and dose-response characteristics
- Potential applications beyond RSE
- Concluding thoughts
Why I care
In a nutshell:
- I embrace the challenges associated with the high-complexity, fast-paced environment of investing in drug R&D
- Investing in healthcare means investing in a healthier, happier and more prosperous future
- Significant unmet need in CNS disorders, personal awareness of some of these conditions through family and friends and the potential for significant near-term advances continue to retain my particular interest
Before proceeding to today’s main topic, a few words for new readers on what motivates me to spend a significant amount of my free time researching healthcare investments.
Investors in the pharmaceutical sector – especially those of us focusing on small, R&D-orientated companies – operate in a high-risk, high-reward environment characterized by constant technological disruption, fierce competition, execution risks, political risks, IP vicissitudes, regulatory uncertainty and many other complications.
Confronting challenges expands knowledge and builds character
The fundamental reason to bother despite of the above is a combination of intellectual curiosity – no biology course can substitute for the mandatory confrontation with emerging science that enables cutting-edge due diligence in biotech – and a drive to turn what is daring or unapproachable for most into something that is thrilling and enriching for myself and through my publications, to my readership.
The profit motive in the pharmaceutical space aligns with positive societal impact
Go around asking and you’ll find no shortage of people with grievances directed towards the pharmaceutical business. It would be foolish to argue that all is dandy, but a sober look is all it takes to realize that we would be living excessively fragile and miserable lives without the significant advances in pharmaceutical development accomplished over the past 150 years.
In my view, nothing is more fundamental to the human endeavor than our individual and collective health, and I can’t think of many investments that would be more rewarding than those that help advance new, impactful medicines.
Cognition is our most precious faculty and investments in the CNS space will pay off in more than one way
Neurological and psychiatric indications continue to present high unmet need and have been a focus of my attention as an independent investor in the pharma / biotech space for the past several years. My interest in the central nervous system (“CNS”) space is driven by a keen awareness of inadequacies in the standard of care (“SOC”) and the satisfaction of seeing meaningful new therapies advanced both for patients suffering from rare, debilitating diseases – children in particular – as well as for the millions struggling with depression, anxiety, dementia and other cognitive & psychiatric impairments.
Fundamental drivers of present and future demand in CNS
Existing unmet need in CNS relates to inadequacy of available therapies whereas emerging unmet need relates to demographics; first and foremost an aging population.
The global cost of treating / caring for patients with Alzheimer’s disease is thought to exceed $1tn, and even this number fails to account for indirect costs such as the unpaid work of caregivers and family and the impact on caregivers’ health((https://content.iospress.com/articles/journal-of-alzheimers-disease/jad190426)).

Other highly challenging conditions such as treatment-resistant depression, schizophrenia and congenital epileptiform and developmental disorders also present significant room for improvement with regards to their SOC and a great need for reduction in the burden of care.
Future return on investment (“ROI”) is set to correlate with high therapeutic unmet need in conditions such as those outlined above.
The challenge of treatment-refractory status epilepticus
In a nutshell:
- RSE entails very high mortality rates and generally poor outcomes
- The current SOC presents a dual dilemma of lacklustre efficacy and significant drug-induced complications
- RSE & SRSE represent a significant burden for ICUs
- Inability to rein in SE makes addressing the underlying condition even harder – a vicious cycle
Treatment-refractory status epilepticus (“RSE”) is a neurological emergency entailing very high mortality rates (around 40%((https://onlinelibrary.wiley.com/doi/epdf/10.1111/epi.12064)) ) within a very short timeframe, as well as costs that significantly exceed the budget allocated to hospitals via the DRG system (average cost of RSE therapy >$50k).
Status epilepticus (“SE”), even before advancing to the treatment-refractory setting, is considered the most extreme and life-threatening occurrence on the spectrum of epileptiform disorders and is defined as a seizure or series of seizures lasting at least 5 minutes((https://onlinelibrary.wiley.com/doi/full/10.1111/epi.13121)). SE is firmly “established” once it exceeds 10 minutes in duration.
RSE is commonly defined as SE that has failed at least one line of therapy, usually hailing from the benzodiazepine class. Super-refractory SE (“SRSE”) is defined as failure to respond to IV anesthetics with recurrence of seizures beyond 24h of treatment initiation.

Here’s a primer on SE by the American Epilepsy Society, highlighting that prolonged seizures can lead to irreversible brain damage, making swift and efficacious intervention critically important:
In simple and obvious terms, then, the primary objective of the management of SE is to stop the seizures with minimal collateral damage to the patient’s vitals. General anesthesia and/or an artificially induced coma need to be avoided, as the latter complicates the task of investigating & addressing the underlying medical condition(s). Artificially induced comas entail a significant risk of death and the dilemma of seizures re-emerging as patients regain consciousness.
The pharmacological standard-of-care in SE consists of IV benzodiazepines such as midazolam, lorazepam and diazepam:

Benzodiazepines are a first choice given their favorable safety profile compared to both older and newer anti-epileptics. I discuss some of these agents further down. While benzodiazepines are highly effective in managing acute seizures (and psychiatric symptoms such as anxiety) thanks to their GABA-ergic mechanism, the synaptic receptors upon which benzodiazepines act can become down-regulated via a variety of mechanisms((https://www.ncbi.nlm.nih.gov/pubmed/8894844)), which are a response to chronic use of benzodiazepines and overstimulation due to prolonged seizures. This helps explain why 1st line benzodiazepines often fail to keep SE under control, requiring additional lines of therapy.
An additional explanation is that benzos primarily act on synaptic GABAa receptors, failing to induce the tonic inhibition((https://www.researchgate.net/profile/Peter_Goldstein/publication/7599854_An_Extrasynaptic_GABAA_Receptor_Mediates_Tonic_Inhibition_in_Thalamic_VB_Neurons/links/55e44cc908aecb1a7cca0732.pdf)) that is likely required for durable seizure control in many SE patients.
New findings around the efficacy of second-line therapy
In a nutshell:
- Hitherto, absence of level 1 evidence meant that there was no agreement around which drugs should be used after benzodiazepines have failed to stop seizures in SE patients
- A new study backed by the National Institute of Neurological Disorders and Stroke provides, for the first time, a high-quality comparison between 3 AEDs for the treatment of RSE
- None of the 3 AEDs provided seizure control at 60 minutes in more than 50% of RSE patients
There is hardly any consensus around what constitutes best practice for the treatment of benzodiazepine-refractory SE. While newer agents such as levetiracetam (“Keppra”) have been introduced & met with significant commercial success – global sales totaled $790m in 20181 – their efficacy in treating benzodiazepine-refractory SE had not been thoroughly evaluated – until now.
A thorough new study backed by the National Institute of Neurological Disorders and Stroke, part of the NHS, was recently published in the NEJM and has been making the rounds. Its key finding is that the three most commonly used anti-epileptics in RSE following benzodiazepine administration have equal, and frankly lacklustre, efficacy.
Measured at 60 minutes after treatment initiation, outcomes across 384 patients were highly similar following the administration of levetiracetam, fosphenytoin or valproate in addition to baseline benzo therapy, each managing to break status in less than half of treated patients (47%, 45% and 46% respectively):

It should be noted that the NIH study only looked at seizure control at 1h post-infusion, whereas RSE patients typically remain in the ICU for more than a week. Despite its limitations, this is the first large-scale, randomized, double-blind trial comparing these three AEDs head-to-head in RSE, and it really drives home the need for better options in RSE.
A separate, equally recent meta-analysis2 provides an additional high-level view on the efficacy of existing SOC across a sample spanning 543 patients. Key findings include:
- Keppra shows similar efficacy (seizure cessation & mortality) as generic phenytoin and generic valproate, while exhibiting a more favorable safety profile (lower risk of poor neurological outcomes, lower need for ventilator assistance)
- However, the addition of Keppra to the benzo clonazepam showed no significant improvement in seizure cessation 15 minutes following treatment initiation when compared to placebo.
The two above-mentioned studies thus strongly suggest that Keppra adds little to the SOC in terms of efficacy, while offering better safety outcomes compared to older drugs.
Physicians discussing the NEJM study on twitter furthermore noted that the high loading doses required for Keppra in SE were only recently established, and that the drug suffers from significant latency (time from infusion to peak efficacy):
Thus, the bar for an improved SOC in SE & RSE is set:
- break status earlier & in a higher % of patients
- induce less neurologic and systemic adverse events
- reduce the need for intubation & prolonged hospitalization
- avoid escalation to anesthetics
Or, in the words of Ruegg et al.:
An ideal AED for these clinical situations would display the following features: no metabolism, no interactions, no sedation, no toxicity, and instantaneous onset of action. Most of the AEDs with an intravenous formulation currently available fail to meet one or more of these requirements and may thereby further complicate the management of critically ill patients.
Swift, durable & safe seizure control across all SE patients, out to several days post-infusion would be nothing short of a revolution in this field, benefitting all stakeholders – patients, treating physicians, healthcare systems and of course the maker of such a miracle drug.
Incidence of SE and RSE
In a nutshell:
- Large studies support an incidence of SE in children and adults corresponding to 46-86k cases / year in the U.S. alone
- Of these, 1/3 can be estimated to progress to RSE, corresponding to 15k-29k cases
- Mortality in the RSE setting is in the 30-40% range
An article by Shorvon & Sen in the October issue of Seizure: European Journal of Epilepsy((https://www.seizure-journal.com/article/S1059-1311(19)30215-8/fulltext)) reviews several high-quality population-based studies to provide a balanced estimate of the incidence of SE in adults.
The 6 studies included for consideration spanned a population of 4 1/2 million across the US and Europe, and defined SE as seizures lasting longer than 30 minutes – a cutoff that has been used as a definition of RSE, suggesting that these studies may not capture all instances of SE. With these criteria, incidence ranged from 10-20/100k per year. Applied to the adult population in the U.S., this yields 20-40k cases annually in the US alone, excluding SE episodes lasting less than 30 minutes and excluding SE in pediatric patients.
In children, the estimated incidence of SE ranges between 18-23/100k per year, with an aggregate mortality rate between 2 and 7%((https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4850470/)). Furthermore, incidence of SE is particularly pronounced in neonates, clocking in at 135-150/100k.
In the aggregate, then, the incidence of SE in the US across adult and pediatric populations can be conservatively estimated to be in the range of 46-86k cases per year. The incidence of RSE is difficult to define with precision, but multiple approaches to ascertaining it (ICD-10 coding, medical literature & market research) point towards at least 1/3 of SE cases being treatment-refractory to first-line benzos, which equals to 15k-29k annual incidents in the U.S.
We can then move one step further and apply outcomes from the previously mentioned, randomized, NIH-funded trial((https://www.nejm.org/doi/full/10.1056/NEJMoa1905795)) of Keppra vs fosphenytoin vs valproate in RSE and ascertain that >50% of RSE cases fail to resolve with the addition of the above-cited 2nd line agents. This translates into roughly 8k-15k RSE patients progressing beyond 2 lines of therapy in the U.S. each year.
This population represents a dramatic and urgent unmet need and as a result, a worthwhile indication for drug development. Mortality in RSE has been estimated at 40% with current SOC, and this was corroborated for instance by a 111-patient study((https://link.springer.com/article/10.1007/s40263-013-0049-y)) testing Vimpat as an add-on to patients whose RSE had not resolved following a median of 2 prior AEDs. Overall mortality rate between both study arms was 30%, and 39% in those who did not receive Vimpat.
Vimpat, like Keppra, is an AED currently marketed by UCB Pharma. Globals sales exceeded $1bn in 2018. The IV formulation of Vimpat is patent-protected until early 2022 in the United States.
A succinct discussion of available 2nd and 3rd line AEDs and their limitations
In a nutshell:
- Commonly used 2nd and 3rd line agents present with a variety of issues such as unfavorable systemic toxicity, drug-drug interactions and severe respiratory depression
- These safety liabilities are often cumulative & need to be managed in their own right on top of the ongoing SE and its underlying medical conditions
- While propofol has a very rapid onset of efficacy, progression to general anesthetics is associated with very poor outcomes
To further ascertain the limitations of current SOC for RSE – beyond the lack of seizure control in a significant portion of patients – I would like to list some of the well-known drawbacks of 4 of the most commonly used 2nd and 3rd line AEDs as well as the anesthetic propofol.
| Name (brand name) | Class | Generic availability (U.S.) | Therapeutic limitations | Notable adverse events / toxicity |
|---|---|---|---|---|
| IV Levetiracetam (Keppra) | Racetam | N | Delayed onset of action | Generally well tolerated. Beyond the usual AEs associated with CNS activity (somnolence, dizziness, weakness etc), moderately increased AEs include incidence of infections. A 2008 study of IV Keppra found that 2 out of 24 SE patients treated with the drug experienced thrombocytopenia (Ruegg et al.) , which might help explain increased susceptibility to infection. |
| Valproic acid (Depakote) | Fatty acid derivative | Y | Larger doses associated with hyperammonemia, liver abnormalities. | Thrombocytopenia and cases of acute encephalopathy as a side-effect of drug-induced hepatic abnormalities (Trinka et al.) |
| Phenytoin & fosphenytoin (Cerebyx) | Hydantoin | Y | - Phenytoin: slow rate of infusion & delayed onset of action. Needs preparation with polypropylene glycol in an alkaline solution, which can entail various injection reactions and even tissue necrosis / extravasation. (Trinka et al.) - Fosphenytoin: 15min conversion time to phenytoin. Costly. Applicable to both formulations: respiratory depression. | High incidence of hypotension (28-50%) paired with cardiac arrhytmias (2%) are of particular worry in patients >50 years. Problematic, as incidence of SE increases significantly beyond 60 years. |
| Topiramate (Topamax) | Sulfamate-substituted monosaccharide | Y | - No IV formulation FDA approved & commercially available - Drug interactions with phenytoin, valproic acid and lamotrigine noted in FDA label - Dose adjustments required in patients with renal impairment | Paresthesia & dose-, age-independent case reports of ocular side effects Royal College of Ophthalmologists |
| Propofol (Diprivan) | Alkyl phenol | Y | Fast onset of action offset by significant evidence pointing to increased mortality rates linked to propofol use in SE (Niermeijer et al.). | Propofol infusion syndrome. Severe respiratory depression. |
The above table is not aiming for perfection: listing all reported off-target effects of these AEDs would exceed the scope of this write-up.
While the general anesthetic propofol rapidly suppresses seizures, it should be reserved for use as a drug of last resort given that it produces significant respiratory depression, bradycardia and can induce a complex and often lethal condition known as “propofol infusion syndrome” when administered over extensive periods (as is typically required in RSE).
Rapid seizure cessation, durable efficacy and lack of systemic toxicity: a paradigm shift is at hand
In a nutshell:
- An IV formulation of the synthetic neurosteroid ganaxolone has yielded near-complete seizure control through 24h and prevented progression to additional AEDs or anesthetics
- Onset of efficacy was near-immediate, “propofol-like”
- This was achieved in a setting with an average of 3 prior lines of therapy. All patients had failed IV Keppra or Vimpat prior to receiving ganaxolone
- The target dose was associated with a significant improvement in CGI scores and shortened hospitalisation
- No off-target toxicities have been identified & sedation was rapidly reversible via dosage adjustments

Data from 17 RSE patients treated with escalating doses of the synthetic neurosteroid ganaxolone, which were announced in late September and which will be presented in more detail at the upcoming American Epilepsy Society annual meeting (“AES 2019”), showed durable efficacy across all three doses studied, with none of the 17 patients requiring escalation to IV anesthetics at 24h. Furthermore, in the high dose, none of the 8 patients treated with IV ganaxolone required additional AEDs or anesthetics at any time through the follow-up period (24h post-taper).
Seizure cessation following the administration of IV ganaxolone (“IV GNX”) occurred within minutes – comparable to that of propofol, while avoiding anesthesia.

As outlined above, these outcomes were produced in a heterogenous population, following the failure of 1st line benzos and, on average, 2 additional IV AEDs.
All patients had failed to respond to Keppra or Vimpat prior to the administration of IV GNX.
The study furthermore measured “real-world” outcomes related to hospitalization and patient disposition at final follow-up. Half of patients receiving the medium dose, and 3/4 of patients receiving the high (=target) dose were able to limit their stay in the intensive care unit (“ICU”) to less or equal than 10 days. For reference; a recently published review3 of 2,585 SE admissions in Germany found a median length of hospitalization of 14 days in RSE, as well as a median 37 days of hospitalization in SRSE.

The dramatic prolongation of ICU stay for patients who progress to SRSE is corroborated by a French study of 78 patients across 10 years and 19 ICUs, published in the journal Critical Care ((https://ccforum.biomedcentral.com/articles/10.1186/s13054-015-0914-9)), which reports a median stay in the ICU of 28 days. It is worth noting that 1/3 of SRSE patients in this sample died from multiple organ failure, highlighting the complications associated with currently available treatments. The study authors conclude that 80% of patients experienced poor outcomes, most patients died from systemic complications linked to their ICU stay and no robust factor of good outcome was identified for the SRSE population.
Most [SRSE] patients died from systemic complications linked to their ICU stay. (Study of 78 PRSE/SRSE patients, Lai et al.)
Inadequate seizure control with 1st line benzos and 2nd / 3rd line AEDs, severe complications associated with escalation to general anesthetics in RSE, and extremely poor outcomes in SRSE patients together cement the significance of the IV GNX data in RSE.
Ganaxolone’s MOA, PK/PD and dose-response characteristics
In a nutshell:
- GNX is a positive allosteric modulator of GABAa receptors involved in tonic inhibition
- GNX exhibits a straightforward dose-response relationship as evidenced in 2 distinct patient populations treated with IV GNX
- The therapeutic window for GNX is significant, the only limiting factor being sedation
- EEG readings help identify the GNX plasma levels required for seizure control in RSE patients
Neurosteroid MOA on GABAa receptors
Ganaxolone is an analog – a near-identical version – of the endogenous (=naturally occurring) neurosteroid allopregnanolone (“allo”). GNX was rationally designed for increased bioavailability over endogenous allo and its oral form has been administered to adult and pediatric patients chronically.

GNX is a positive allosteric (=indirect) modulator of GABAa receptors, binding to a molecular pocket that is distinct from those targeted by benzos and barbiturates. Early preclinical studies showed that GNX potentiates the activity of benzos and other potent GABAa modulators((http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.963.1290&rep=rep1&type=pdf)). Combination of ganaxolone with clonazepam – a commonly used benzo – has yielded supra-additive anxiolytic effects in rat behavioral studies((https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6334648/pdf/nihms-1004144.pdf)), and prior to the RSE readout in patients, preclinical studies showed that benzos and GNX exert synergistic anti-epileptic effects.
These synergies can be partially explained by the different GABAa receptor subtypes modulated by benzos and neurosteroids. Another plausible explanation – complementary to the aforementioned – is that the combined action of neurosteroids and benzos is greater than the sum of its parts for mechanistic reasons. Let’s have a closer look at the way neurosteroids interact with GABAa receptors on the molecular level:

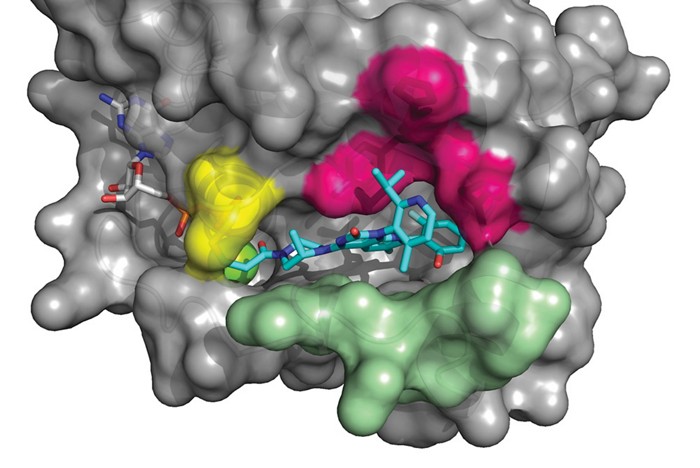
Publishing in the Nov. 2017 issue of Nature Structure & Molecular Biology((https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6166781/)), a team of European researchers overcame limitations to the expression of macromolecular protein assemblies by producing a chimeric GABAa receptor construct and proceeding to structural analysis and molecular modeling.
Their research suggests that neurosteroids bind at an inter-subunit location of the receptor’s transmembrane domain (“TMD”), as opposed to the benzos, which bind to pockets in the receptor’s extracellular domain((https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3127544/)).
This in turn leads to a distinct conformational change, which can be described simplistically as a subtle outward pull on the receptor’s desensitisation gate. This conformational change renders GABAa receptors more susceptible to activation by ambient GABA (=potentiation).
Furthermore, it has been suggested that neurosteroids can lead to direct activation of GABAa receptors on their own via simultaneous binding to 2 discrete transmembrane sites((https://www.ncbi.nlm.nih.gov/pubmed/17108970)).
Properties of IV GNX
To enable its IV administration, GNX is conjugated with the same proprietary cyclodextrin that has enabled the development of allo into an IV therapy for post-partum depression (“PPD”) under the trade name Zulresso.

Captisol, as this proprietary cyclodextrin is called, benefits from a safety record spanning two decades. A dozen FDA-approved drug products are formulated with it.
The IV formulation of GNX has been tested in two patient populations to date: PPD & RSE.
In both indications, a dose-response was evident, with higher doses inducing stronger anti-depressant and anti-epileptic effects. The below graphics show efficacy observed with the highest dose tested in PPD & the modeled PK curves for the 3 doses tested in RSE, respectively.


N.b.: The anti-depressant properties of GNX merit a separate discussion. For the purposes of the present article it is simply worth noting that infusions of the drug at doses much lower than those deployed for RSE have consistently yielded anti-depressant effects that separate from placebo as early as 6h after initiation of therapy. The dataset generated in PPD strongly suggests that both the dose and the length of infusion play a significant role in maintaining these anti-depressant effects over time.
At AES 2019, the company is presenting in-depth findings linking seizure control & normalization of EEG readings in RSE with plasma GNX levels >500ng/ml((https://www.aesnet.org/meetings_events/annual_meeting_abstracts/view/2421131)). At the target dose >700mg/day, GNX plasma levels were maintained above 500ng/ml for roughly 8 hours, which translated into 0/8 patients requiring escalation to additional AEDs or anesthetics throughout the follow-up period, as discussed earlier.

GNX has been tested in >1600 subjects, at oral doses regularly reaching 1800mg/day and now at high doses via IV. Throughout its history, GNX has exhibited a “clean” safety profile, displaying no off-target side effects. At the high doses employed in RSE on top of several prior lines of therapy including IV benzos, severe sedation crops up, but is reversible via dose-adjustment. The available evidence shows that GNX benefits from a remarkably large therapeutic window, providing patients and physicians with significant flexibility in their treatment choices.
Potential applications beyond RSE
Additional uses as an IV anti-epileptic
The strong and unequivocal dataset in RSE supports use of the drug earlier in the treatment algorithm (immediately following benzos) and potentially in SRSE. By the same token, IV GNX could prove superior over SOC as a prophylactic anti-convulsant treatment following neurosurgery((https://www.ncbi.nlm.nih.gov/pmc/articles/PMC321029/)). Finally, infantile spasms are associated with neurocognitive delays and there is a lack of high-quality evidence in support of a therapy of choice((https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4728997/)).
Severe depression
Outcomes of 2 PhII trials in postpartum depression and of an independent, investigator-led trial in treatment-resistant depression((https://www.clinicaltrials.gov/ct2/show/results/NCT02900092)) support further development of IV (and oral) GNX in these indications. Outcomes with Zulresso and to a lesser extent zuranolone((https://en.wikipedia.org/wiki/Zuranolone)) lend credibility to a GABAergic hypothesis of depression.
Neurodegenerative disease
A body of preclinical research supports the use of intermittent neurosteroid therapy for the treatment of Alzheimer’s Disease and Parkinson’s Disease((https://www.frontiersin.org/articles/10.3389/fncel.2014.00203/full)). Researchers found that such intermittent doses “increased hippocampal neurogenesis, increase neural progenitor cell survival, and reverse learning and memory deficits, decreased microglial activation, and decreased amyloid-beta pathology“.
Ongoing trials
An oral formulation of ganaxolone is currently being evaluated in 2 PhIII trials in children with rare genetic epileptiform and developmental disorders: CDKL5 deficiency disorder((https://www.clinicaltrials.gov/ct2/show/NCT03572933?cond=cdkl5&draw=2&rank=1)) and PCDH19 female epilepsy((https://www.clinicaltrials.gov/ct2/show/NCT03865732?cond=pcdh19&draw=2&rank=1)).
Long-term, significant seizure reductions >50% from baseline have been previously reported for CDKL5 patients receiving oral GNX up to 1800mg/day((https://www.aesnet.org/meetings_events/annual_meeting_abstracts/view/506062)).
The PhIII trial in PCDH19 is the first-ever epilepsy trial to be stratified on the basis of a predictive biomarker (allopregnanolone-sulfate or “allo-s” for short). Low levels of allo-s have been strongly correlated with response to oral GNX in prior testing((https://www.aesnet.org/meetings_events/annual_meeting_abstracts/view/502507)).
Concluding thoughts
The pursuit of better treatments for lethal & debilitating conditions such as RSE, treatment-resistant depression and developmental disorders combines an economic rationale with a higher purpose.
IV GNX has demonstrated paradigm-changing efficacy and safety outcomes in RSE, and data generated in PPD cross-validate the drug’s PK/PD, dose response and therapeutic window.
Additional indications for IV GNX could include treatment-resistant depression – similarly to how IV ketamine is currently used off-label in specialized infusion centers – and even neurodegenerative conditions.
Ongoing trials of oral GNX offer hope for children suffering from treatment-resistant seizures and severe developmental disorders.
- https://www.prnewswire.com/news-releases/ucb-full-year-report-2018-2018-marks-the-fifth-consecutive-year-of-profitable-growth-intensifying-investment-in-ucbs-strong-pipeline-300804398.html [↩]
- https://www.sciencedirect.com/science/article/abs/pii/S1059131119301530 [↩]
- https://onlinelibrary.wiley.com/doi/full/10.1111/epi.13837 [↩]
Great summary of the state of affairs in RSE. Very informative. Thanks Jerome.
Great work Jerome, appreciate all of your efforts. Very exciting…
Thanks for the article,great read.This little company is going to have an incredible comeback and have a positive change in many people’s lives.It is great to follow an author that is consistent,serious and responsible with is writtings;not just chasing the latest thing.As for alzheimer,a huge unmet need,i would like to bring to your attention results from Cassava sciences,very compeling and mostly funded by nih.If you have time and interest this one may be worthy of your research.
Good luck to all!